
European CTC Implementation Guide
Introduction: European CTC Implementation Guide
The CTC-EU-Network aims to make the established CTC-method transferable to other European countries.
This European Implementation Guide will facilitate the use of the CTC-method in other European countries. Evaluations of CTC are showing positive impacts for children living in the CTC-area, compared with children who did not live in the area. The EU-funded CTC-EU project (2013-2015) contributes to enhanced implementations of community-based programmes based on a risk and protective factor model, and initiatives that focus on preventing the development of problem behaviour by early intervention with children and youth.
The project results lead to a facilitated use of the "Communities That Care" approach by stakeholders in community-based prevention efforts (municipalities, youth-care agencies, schools and preschools, parents etc.). Thus, beneficiaries of the project will be after all families and youth in communities who use the CTC framework to increase the implementation of evidence-based prevention measures, taylored to their local specific needs and resources.
Our project aims to facilitate the implementation of the CTC-system in every European country. We expect that adapting CTC from the U.S. is only in part adapting it to specific national conditions, but at the same time (even more) adapting it to European conditions. Based on the expected results of our project this work could be economized in future.
Implementing CTC measures at the European level will reduce implementation costs for communities and states. CTC itself has been found a cost-beneficial intervention in the U.S. (5,3 $ return on every 1 $ spend, Kuklinski et al. 2011).

What is CTC?
Communities That Care (CTC), a coalition-based system for preventing a wide range of adolescent problem behaviours, was developed by J. David Hawkins and Richard Catalano of the Social Development Research Group to narrow the gap between science and community priorities and practices.
CTC core elements are:
- Social epidemiological analysis of problem behaviours in a community (social background, problems, risk factors and protective factors),
- Worked out implementation strategy (trainings, guidance, community actors, implementation over time),
- Use of effective and tested programs,
- Evaluation of results and ongoing strategy.
The CTC-approach involves assessing the prevalence of problem behaviours, but also of the risk and protective factors in a community (e.g. a neighbourhood, city borough or town) related to the problem behaviours. With the local profile based on epidemiological research on problem behaviours, risk factors and protective factors, communities can identify and choose tested and effective, preventive interventions to address these underlying factors. A strategic, community specific process has been designed and tailored to increase communication, collaboration and ownership among professionals, service providers and community members. During this process, communities get technical assistance and specific training courses by trained and licensed CTC-experts. Although it is a community intervention in which different parties bear responsibility, one person (the local project leader or coordinator) has specific responsibilities during the three year implementation period. After the implementation period, the community will be strong enough to work on its own, using the CTC-prevention framework.
The originality of CTC lies in its rationale and systematic approach of social and youth problems at the local level. Social change is a very complex process and it requires a well thought through and reasoned approach through knowledge of the problems at hand, reliable organisation and the availability of effective interventions.
CTC consists of 5 phases:
5 Phases of CTC
Communities That Care is an ongoing process. When communities follow the phases below, their young people get improved conditions to flourish.
- Get Started
Communities get ready to introduce CTC. They work behind the scenes to:- Activate a small group of catalysts.
- Assess how ready the community is to begin the process.
- Identify key community leaders to champion the process.
- Invite diverse stakeholders to get involved.
- Get Organized
Communities form a board or work within an existing coalition. After recruiting community board members, they:- Learn about prevention science.
- Write a vision statement.
- Organize workgroups.
- Develop a timeline for installing CTC.
- Develop a Community Profile
Communities assess community risks and strengths—and identify existing resources. The community board and workgroups:- Review data from the community’s youth survey.
- Identify priority risk and protective factors that predict targeted health and behavior problems.
- Assess community resources that address these factors.
- Identify gaps in existing resources to be filled in.
- Create a Community Action Plan
The community board creates a plan for prevention work in their community, to:- Reduce widespread risks and strengthen protection.
- Define clear, measurable outcomes using assessment data.
- Select and expand tested and effective policies and programmes using the Blueprints for Healthy Youth Development website (in the U.S.).
- Implement & Evaluate
In this final phase, communities:- Implement selected programmes and policies.
- Monitor and evaluate them.
- Measure results and track progress to ensure improvements are achieved.
CTC in Europe
Introduction of CTC (reasons and expectations)
The following information is based on the data given by the participating countries. In the report ‘CTC in Europe 1998-2015, overview and experiences´(March 2016) detailed information of each of the participating countries can be found. Clickable link report
There are three main reasons why countries in Europe started with CTC. There are problems and issues with:
- Effectiveness of Youth Policy. To improve evidence-based prevention as a way of working (and improve policy with science (‘data-driven’) and the promoting the development and use of evidenced based programmes (EBP).
- Policy/Institutional. In all countries, there was a situation in which the cooperation between the government and other institutions involved could be (or should be) improved. There was a desire to create stronger coalitions both vertical and horizontal, on a national level, but also locally (mobilize local communities).
- Youth. And of course, the reduction youth problems such as:
- Alcohol- and drugs abuse
- Aggression and violence (in schools)
- Truancy, school failure
- Family management problems
The expectations of what CTC could bring were usually high, e.g.:
- Framework for promotion and implementation of prevention,
- Platform for cooperation,
- Rational use budgets/cost-effectiveness,
- Ongoing professional empowerment,
- Grounded policy decisions,
- Bridge between practise and science,
- More sustainable methods/ebp’s,
- Stronger local coalitions (CTC Community Boards),
- Better youth, stronger families, less problems
Although it varies between countries who took the initiative to introduce CTC, we could identify a “Triple Helix of CTC” in terms of a cooperation between 1) government, 2) universities / science and 3) intermediary institutions as a success formula for introducing CTC in a country.
|
|
Initiative to start with CTC |
In cooperation with: |
|
Cyprus |
University |
Local Government |
|
Croatia |
University |
Local Government |
|
Germany |
State Government |
University |
|
Austria |
Institution |
|
|
Sweden |
Local Government |
National Government |
|
UK |
Institution |
University |
|
Netherlands |
National Government |
Institution |
|
Switzerland |
Institution |
Issues and Experiences
Within the countries different implementation strategies were used. Often it was a combination of:
- Creating a coalition for prevention (national, local)
- Funding (national/state, no or little local costs)
- ‘Formal’ agreements
- Pilots (guided introduction)
- Use of good examples
- Information (websites, use of survey results)
- Activities (conferences, sharing knowledge)
Of course, there was also some hindrance and challenges. Often mentioned was:
- CTC is very American and therefore not suitable in this country.
- CTC is too theoretic, too complicated and too hard to explain to practitioners and local government.
- It takes too long to get/see results. Difficult to keep organisations and people committee over time.
- Prevention is no part of the job description of cordinators (second task, no time).
- No community readiness (lack of willing decision makers, or competent project leaders).
- CTC is a standard method that is in conflict with established individual professionalism.
- Competition with other efforts/programmes.
The process evaluation studies (see also Further Reading) offer four groups of factors that influence the implementation of CTC:
Cooperation issues:
- Lack of important partners in the coalition (e.g. schools).
- Not enough involvement of non-professional community members.
- Sustainability of the involvement of residents.
Boundary issues:
- Different working areas for different organisations.
- Differences in living- and school area of youth.
Quality issues:
- Coordinator- and staff turnover.
- Insufficient resources for action plan.
- Lack of evidence of CTC success.
Positioning issues:
- Unclear relationship of the CTC effort to other (community-based) initiatives.
- Complexity of youth policy field.
- Change of policy.
Supportive for the quality of CTC-implementation were:
- Certified trainers.
- Local coaching for projectleaders & training teams.
- Technical assistance.
- Milestones & benchmarks checklist for process guidance.
- National survey as benchmark data for the local data assessment.
- 5 phases for implementation.
- Adequate funding.
Conclusions
In the graphic below the numbers of CTC-sites per country are shown in the period 1998 – 2015. This is based on the available data given by the participating countries. In the report ‘CTC in Europe 1998-2015, overview and experiences´(March 2016) detailed information of each of the participating countries can be found. Clickable link report
In total there are more than 100 sites where CTC was implemented. Very often ‘deprived’ areas with low income population, above average problem behaviours and elevated risk factors. In cities as well as in rural areas, in small villages with 2000 inhabitants and in large areas with over 100.000 inhabitants CTC was implemented.
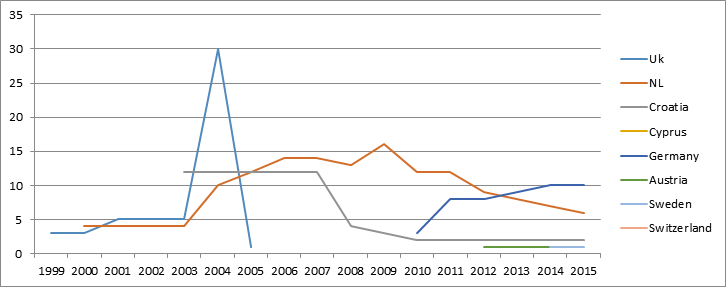
But as the graphic also shows in 2015 only 20 sites are still working with CTC. In the Netherlands, the United Kingdom and Croatia (together the early adopters of CTC) CTC grew very rapidly in the beginning, but at this time it is no longer an extensive part of youth policy in those countries.
Formula E=QxA
It shows that the Effectiveness of CTC in the EU context is currently not very high.
This is not neccessary a problem with the Quality of CTC. CTC as a meta-programme is widely recognized as valuable. The core elements of CTC: youth survey, evidenced based programs, PDCA cycles, training etc. make it a sound and qualitative good approach. Of course, some improvements of implementation are possible, but they do not affect the core elements of CTC.
The Acceptence seems to be more problematic. It differs per country, but overall there are a few reasons given why this needs more attention in the future.
CTC implementation is not possible only on a local level. Research, establishing a survey baseline, a menu of evidence-based programs and training/coaching are too complex and too costly for only the local level. Lasting involvement on a ‘higher’ governmental level is necessary. CTC implementation demands coalitions on local AND national level.
- Between local and national prevention policy
- Between academic knowledge and local application
- Between different support organisations
Sustainable implementation of prevention policy requires sustainable commitment of the key-players: government, universities and professional intermediary institutions on different levels (national, state, local). Sustainable commitment means: long term (15-20 years), funding for the essential infrastructure, and maintaining the priority for prevention.
Regarding CTC it means longitudinal youth surveys, ongoing work on evidence-based programmes and sufficient training and coaching, separate and in combination.
Implementation of CTC means in a way a system change. Not enough awareness of the complexity this brings in will influence the effectiveness. Underestimating this complexity will lead to disappointment.
Guidelines for Implementing CTC in European Context.
Meso and macro level implementation actions need to be considered.
CTC related issues on this level are: youth surveys/ databank/menu of evidence-based programmes and training on acceptance are having local implications.
At a national level, countries starting with the implementation of CTC should take a close look at the country readiness. In this paragraph, we first consider local issues and from there we elaborate on the concept of country readiness.
Make arrangements for reliable data collection on risk and protective factors and problem behaviours, which can be repeated over time.
Youth Survey:
A challenge with the CTC youth survey is to get and keep the involvement of local schools involving the age group 12-18 years old. They are in some cases not willing to cooperate. In case of inviting youth to fill in the survey online by sending an invitation at their homes the problem is a lack of response and non-response of groups at risk, impairing the validity of the youth survey results. If this happens acceptance of CTC is endangered. Building long-term trusting relationships with school administration and principals is key.
Know what programmes are involved in the community and develop knowledge and acceptance of better fitting evidence based programmes
Programme Databank:
Generally on a national level databanks/ menues of evidence based programmes are accepted and embraced as showing what should be done. But on a local level it means that professionals should be trained in new programmes, that type of costs of introducing new programmes should be taken in account for. Another form of resistance to implementing evidence based programs is the fear to stop with an already established programme/activity done for years, which is felt as a rejection of tacit professional knowledge and experience. This results often in claiming that the usual activities will show evidence if researched anyway, but for that local funds are too small or not available.
Make the CTC method and prevention principles largely and repeatedly known during years
Training:
One of the issues often mentioned in the different countries is staff turnover. The people working in the CTC area and involved in the introduction of CTC are very often not the same two or three years later. New people need to be trained in the CTC method and in the science-base of prevention. A change of project leader of CTC seems quite negative for the sustainability of the CTC process.
Keep multi stakeholder management clearly focused on the desired prevention outcomes
Staff:
Trained CTC project leaders should keep the multi stakeholders of the CTC effort informed, connected and involved. This is an arduous task because prevention outcomes appear not directly but after 2-5 years after introducing CTC (Fagan et al, 2008, Quinby et al, 2008)
Local implementation cannot succeed without country-readiness for the implementation of CTC
Country readiness
The CTC approach has extended attention for the community- and stakeholder readiness in the first phase of CTC. In the introduction phase efforts take place to involve the community in prevention science, the underlying theories of the social development model and joint thinking about the “why” of starting with CTC in that particular area.
There is yet no such way of thinking and introducing CTC when a country wants to implement CTC in different communities or cities.
Why country readiness for CTC is important and a condition for successfully local CTC implementation:
- CTC implementation is not possible only on a local level.
- Research, survey baseline, evidence based programmes and training/coaching are too complex and too costly for the local level to organise.
- “Higher” level involvement is necessary: Policy and Government at a national level: for setting the framework of science based prevention, for setting the legislation of local prevention and for funding.
- Knowledge: Universities to develop the science base of prevention on national and regional level.
- Quality of implementation support (training, coaching and technical assistance) is key.
- Larger scale implementation is more cost effective.
Aspects of country readiness:
Organise cooperation between national agencies and universities for development of national CTC instruments: youth survey, databank of evidence based programmes and support: coaching and training
An organisation starting with CTC in a country must make sure that the national (or regional, as in Germany) government supports CTC long enough to realize a system change. A system change is required in the sense of building science based prevention organised at a local level by local CTC implementations that are supported by national agencies for the youth survey (quality, baseline comparison) and a databank of evidence based programmes with tested and available programmes to bring into local settings to target selected risk- and protective factors.
Keep the focus on prevention, reduction of risk factors and promotion of protective factors
The situation of CTC in the Netherlands showed that CTC is vulnerable for policy change on a national level. In the nineties, the national government favoured CTC as a new and evidence based way of organizing prevention and solving the problem of fragmentation in the field of youth policy. In the 2005 the national policy forced local communities to form new organisations for families to receive prevention (Family Centres Centra voor Jeugd en Gezin) that made all the local efforts go to this new organisation and move away from the CTC implementation, even cities that had started implementing CTC stopped because of the need for organizing the family centres. From 2014 onwards with the decentralisation of youth care in the Netherlands, the family centres are now being dissolved in new organisations on a local level. This process costs so much energy and new ways of cooperation that no city is at the moment open to science based prevention as is conducted with CTC.
Organise coalitions:
CTC implementation demands coalitions on local and national level.
- Between local and national prevention policy
- Between academic knowledge and local application of prevention science and implementation science
- Between different support organisations for families, youth, youth care, education and communities
European level
Evaluate CTC implementation in the European context (EMCDDA paper 2017).
Coordinate a community of local CTC project leaders on a European level.
Develop standards of support needed to successfully implementing CTC on national and local level.
Organise a support structure for countries starting with CTC, by learning from experienced countries.
SPAN http://www.span-europe.eu/prevention-science could take an active role in supporting local CTC implementation.
EUSPR could broaden and disseminate knowledge on prevention and the support of well-being in communities based on the CTC methodology. The European Society for Prevention Research promotes the development of prevention science, and its application to practice so as to promote human health and well-being through high quality research, evidence based interventions, policies and practices: http://euspr.org/
EMCDDA has an overview of evidence based interventions in Europe on different levels that will be enhanced by the results of the CTC-EU project on effective preventive interventions available in Europe.
National level
Make the CTC youth survey outcomes part of regular national outcome data. In order to do so organise the CTC youth survey development (translation, reliability and validity assessment and improvement) in the hands of a national accepted university and sustain the youth survey for at least 12 years (3 CTC cycles) to give CTC a chance to show the hoped-for changes in risk and protective factors.
Organise information exchange between local CTC implementation and the government, and national agencies working on prevention.
Keep the science base of prevention in mind and help key leaders to uphold this base of prevention.
Keep universities involved in research on the outcomes of the CTC-youth surveys, including national benchmarks of risk, protective factors and problem behaviours.
Keep national agencies and universities involved in development of databanks with evidence based programmes.
Organise together with research institutes experimental evaluations of local promising programmes.
Organise the professional training and coaching of local CTC project leaders on a national level.
Make the “Triple-Helix” on CTC implementation a standard of national support of local prevention initiatives.Local level
Position the local CTC project leader in the local government. He should be in close contact with aldermen, and decision makers on the local level. One could say the project leader needs a lot of political capital to help the community to stay the CTC track.
Ownership of CTC on a local level should be in the hands of the residents of a community, so that they influence the local agenda and policy making. Develop locally strong co-creation between the professionals and the local community.
Follow the 5 phases of CTC implementation.
Apply the CTC Milestones and Benchmarks for local progress.
Keep the local coalition alive.
How to start with CTC
European level
- Collect information and organise support from international agencies.
- Collect lessons from experienced CTC coaches and trainers from other countries.
- Support national governments with knowledge and training in the conditions of successful CTC implementation and the lessons learned in Europe.
National level
Create a coalition of government departments, universities and national agencies that:
- Translate the CTC methodology fitting in the national culture and adoptable by local institutions and communities.
- Translate and adopt the CTC Youth Survey.
- Start by collecting information on available evidence based programmes, and make these accessible in online databanks.
- Start by selecting and supporting one to four pilot communities willing to implement CTC as forerunners, evaluate their attainments and challenges for further learning.
- Train CTC coaches and trainers.
Local level
- Start a local CTC pilot community within in bigger area.
- Position the local CTC project leader high.
- Organise the data collection by implementing the youth survey.
- Follow the CTC methodology.
- And adopt the local lessons learned in the CTC pilots for making a better fit of the CTC methodology to the regional and national developments.
- Make use of national agencies and universities, build long-lasting collaborative relationships.
Further Reading
Arthur, M.W., Hawkins, J.D., Brown, E.C., Briney, J.S., Oesterle, S. and Abbott, R.D. (2010), ‘Implementation of the Communities That Care prevention system by coalitions in the community youth development study’, Journal of Community Psychology, 38(2), pp. 245-258.
Axford, N., Sonthalia, S., Wrigley, Z., Webb, L., Mokhtar, N., Brook, L., Wilkinson, T. et al. (2016), What works in Europe? Developing a European Communities that Care database of effective prevention programmes, Dartington Social Research Unit, Dartington, UK.
Bannister, J. and Dillane, J. (2005), Communities That Care: An Evaluation of the Scottish Pilot Programme, Social research Crime and Criminal Justice Research Findings No.79/2005.
Basic, J. (2015), ‘Community mobilization and readiness: planning flaws which challenge effective implementation of “Communities that care” prevention system’, Substance Use & Misuse 50(8-9), pp. 1083-1088.
Briney, J.S., Brown, E.C., Hawkins, J.D. and Arthur, M.W. (2012), ‘Predictive validity of established cut points for risk and protective factor scales from the Communities That Care youth survey’, Journal of Primary Prevention 33(5-6), pp. 249-258.
Brown, E.C., Hawkins, J.D., Arthur, M.W., Briney, J.S. and Abbott, R.D. (2007), ‘Effects of Communities That Care on prevention services systems: findings from the community youth development study at 1.5 years’, Prevention Science 8(3), pp. 180-191.
Brown, E.C., Graham, J.W., Hawkins, J.D., Arthur, M.W., Baldwin, M.M., Oesterle, S., Briney, J.S. et al. (2009), ‘Design and analysis of the Community Youth Development Study longitudinal cohort sample’, Evaluation Review 33(4), pp. 311-334.
Brown, L.D., Feinberg, M.E. and Greenberg, M.T. (2010), ‘Determinants of community coalition ability to support evidence‑based programs’, Prevention Science 11(3), pp. 287-297.
Brown, E.C., Hawkins, J.D., Arthur, M.W., Briney, J.S. and Fagan, A.A. (2011), ‘Prevention service system transformation using Communities That Care’, Journal of Community Psychology 39(2), pp. 183-201.
Brown, E.C., Hawkins, J.D., Rhew, I.C., Shapiro, V.B., Abbott, R.D., Oesterle, S., Arthur, M.W. et al. (2014), ‘Prevention system mediation of Communities That Care effects on youth outcomes’, Prevention Science 15(5), pp. 623-632.
Brown, L.D., Feinberg, M.E., Shapiro, V.B. and Greenberg, M.T. (2015), ‘Reciprocal relations between coalition functioning and the provision of implementation support’, Prevention Science 16(1), pp. 101-109.
Burkhart, G. (2013), North American drug prevention programs: are they feasible in European cultures and contexts?, European Monitoring Centre for Drugs and Drug Addiction, Publications Office of the European Union, Luxembourg. Crow, I. & France, A. (2001) CTC—The Story So Far, an Interim Evaluation of Communities thatCare (York, Joseph Rowntree Foundation)
Butterfoss, F.D. (2006), ‘Process evaluation for community participation’, Annual Review of Public Health 27, pp. 323-340.
Catalano, R.F. and Hawkins, J.D. (1996), ‘The social development model: a theory of antisocial behavior’, pp. 149-197, in Hawkins J.D. (ed.), Delinquency and crime: current theories, Cambridge University Press, New York.
Chinman, M., Hannah, G., Wandersman, A., Ebener, P., Hunter, S.B., Imm, P. and Sheldon, J. (2005), ‘Developing a community science research agenda for building community capacity for effective preventive interventions’, American Journal of Community Psychology 35, pp. 143-157.
Crow, I., France, A., Hacking, S., and Hart, M. (2004), Does Communities that Care work? An evaluation of a community-based risk prevention programme in three neighbourhoods. Rowntree Foundation London UK.
Dijk, van A.G., Geldorp, M., Tulner, H. (2002) Tussenrapportage evaluatie vier pilotprojecten CTC DSP, Amsterdam
Doĝan, G., Huygen, A., Mak, J., Steketee, M. (2006), Communities that Care in de praktijk. Beschrijving van vijf pilotprojecten. Verwey-Jonker Instituut, Utrecht.
DSP, (2004), Eindrapportage vier pilotprojecten CtC Amsterdam, Arnhem, Rotterdam, Zwolle. DSP Amsterdam
European Monitoring Centre for Drugs and Drug Addiction (2017), Communities That Care (CTC): a comprehensive prevention approach for communities, EMCDDA Papers, Publications Office of the European Union, Luxembourg.
Fagan, A.A., Hawkins, J.D., and Catalano, R.F. (2008), ‘Using community epidemiologic data to improve social settings: the Communities That Care prevention system’, in Shinn, M. and Yoshikawa, H. (eds), Changing schools and community organizations to foster positive youth development, Oxford University Press, New York (available at
Fagan, A.A., Hanson, K., Hawkins, J.D. and Arthur, M. (2009), ‘Translational research in action: implementation of the Communities That Care prevention system in 12 communities’, Journal of Community Psychology 37(7), pp. 809-829.
Fagan, A.A., Arthur, M.W., Hanson, K., Briney, J.S. and Hawkins, J.D. (2011), ‘Effects of Communities That Care on the adoption and implementation fidelity of evidence‑based prevention programs in communities: results from a randomized controlled trial’, Prevention Science 12(3), pp. 223-234.
Fagan, A.A., Hanson, K., Briney, J.S. and Hawkins J.D. (2012), ‘Sustaining the utilization and high quality implementation of tested and effective prevention programs using the Communities That Care prevention system’, American Journal of Community Psychology, 49(3-4), pp. 365-377.
Faggiano, F., Minozzi, S., Versino, E. and Buscemi, D. (2014), ‘Universal school based prevention for illicit drug use’, Cochrane Database of Systematic Reviews 12, CD003020, doi: 10.1002/14651858. CD003020.pub3.
Fairnington, A., (2004), Communities that care: a case study of regeneration from Wales Critical Public Health, Volume 14, Issue 1, 2004, Special issue: Building multidisciplinary public health in the UK. Taylor & Francis
Feinberg, M.E., Greenberg, M.T., Osgood, D.W., Sartorius, J. and Bontempo, D. (2007), ‘Effects of the Communities That Care model in Pennsylvania on youth risk and problem behaviors’, Prevention Science 8(4), pp. 261-270.
Feinberg, M.E., Jones, D., Greenberg, M.T., Osgood, D.W. and Bontempo D. (2010), ‘Effects of the Communities That Care model in Pennsylvania on change in adolescent risk and problem behaviors’, Prevention Science 11(2), pp. 163-171.
Foster Fishman, P.G., Berkowitz, S.L., Lounsbury, D.W., Jacobson, S. and Allen, N.A. (2001), ‘Building collaborative capacity in community coalitions: a review and integrative framework’, American Journal of Community Psychology 29, pp. 241-261.
Green, L., Daniel, M. and Novick, L. (2001), ‘Partnerships and coalitions for community based research’, Public Health Reports 116, pp. 20-31.
Gloppen, K.M., Arthur, M.W., Hawkins, J.D. and Shapiro, V.B. (2012), ‘Sustainability of the Communities That Care prevention system by coalitions participating in the Community Youth Development Study’, Journal of Adolescent Health 51(3), pp. 259-264.
Haggerty, K.P. and Shapiro, V.B. (2013), ‘Science based prevention through Communities That Care: a model of social work practice for public health’, Social Work in Public Health 28, pp. 349-365 (available at http://doi.org/10.1080/19371918.2013.774812).
Hall, W. (2015), ‘What has research over the past two decades revealed about the adverse health effects of recreational cannabis use?’, Addiction 110, pp. 19-35.
Harachi, T.W., Ayers, C.D., Hawkins, J.D., Catalano, R.F. and Cushing, J. (1996), ‘Empowering communities to prevent adolescent substance abuse: process evaluation results from a risk- andprotection focused community mobilization effort’, Journal of Primary Prevention 16(3), pp. 233- 254.
Hawkins, J.D. and Catalano, R.F. (2002), Investing in your community’s youth: an introduction to the Communities That Care system, Channing Bete Company, South Deerfield, MA.
Hawkins, J.D. and Weis, J.G. (1985), ‘The social development model: an integrated approach to delinquency prevention’, Journal of Primary Prevention 6, pp. 73-97.
Hawkins, J.D., Catalano, R.F. and Arthur, M.W. (2002), ‘Promoting science based prevention in communities’, Addictive Behaviors 27, pp. 951-976.
Hawkins, J.D., Kosterman, R., Catalano, R.F., Hill, K G. and Abbott, R.D. (2008a), ‘Effects of social development intervention in children fifteen years later’, Archives of Pediatric & Adolescent Medicine 162, pp. 1133-1141.
Hawkins, J.D., Catalano, R.F., Arthur, M.W., Egan, E., Brown, E.C., Abbott, R.D. and Murray, D.M. (2008b), ‘Testing Communities That Care: the rationale, design and behavioral baseline equivalence of the community youth development study’, Prevention Science 9(3), pp. 178-190.
Hawkins, J.D., Brown, E.C., Oesterle, S., Arthur, M.W., Abbott, R.D. and Catalano, R.F. (2008c), ‘Early effects of Communities That Care on targeted risks and initiation of delinquent behavior and substance use’, Journal of Adolescent Health, 43(1), pp. 15-22.
Hawkins, J.D., Oesterle, S., Brown, E.C., Arthur, M.W., Abbott, R.D., Fagan, A.A. and Catalano, R.F. (2009), ‘Results of a type 2 translational research trial to prevent adolescent drug use and delinquency: a test of Communities That Care’, Archives of Pediatrics & Adolescent Medicine 163(9), pp. 789-798.
Hawkins, J.D., Oesterle, S., Brown, E.C., Monahan, K.C., Abbott, R.D. and Arthur, M.W. (2012), ‘Sustained decreases in risk exposure and youth problem behaviors after installation of the Communities That Care prevention system in a randomized trial’, Archives of Pediatrics & Adolescent Medicine 166(2), pp. 141-148.
Hawkins, J.D., Oesterle, S., Brown, E.C., Abbott, R.D. and Catalano, R.F. (2014), ‘Youth problem behaviors 8 years after implementing the Communities That Care prevention system: a community randomized trial’, JAMA Pediatrics 168(2), pp. 122-129.
Hemphill, S.A., Toumbourou, J.W., Herrenkohl, T.I., McMorris, B.J. and Catalano, R.F. (2006), ‘The effect of school suspensions and arrests on subsequent adolescent antisocial behavior in Australia and the United States’, Journal of Adolescent Health 39(5), pp. 736-744.
Higgins, J.P.T. and Green, S. (eds.) (2011) Cochrane handbook for systematic reviews of interventions, version 5.1.0, The Cochrane Collaboration (available
Huygen, A., Mak, J., Steketee, M. (2009) Communities that Care in de Praktijk. Beschrijving van de locaties Maassluis, Hoogvliet en Leiden-Stevenshof. Verwey-Jonker Instituut, Utrecht.
Jasuja, G.K., Chou, C.P., Berstein, K., Wang, E., McClure, M. and Pentz, M.A. (2005), ‘Using structural characteristics of community coalitions to predict progress in adopting evidence based prevention programs’, Evaluation and Program Planning 28, pp. 173-184.
Jones, L., Hughes, K., Atkinson, A.M. and Bellis, M.A. (2011), ‘Reducing harm in drinking environments: a systematic review of effective approaches’, Health & Place 17(2), pp. 508-518.
Jonkman, H., Junger-Tas, J., and van Dijk, A. G. (2005), From behind Dikes and Dunes. CHILDREN & SOCIETY VOLUME 19 (2005) pp. 105–116
Jonkman, H., Haggerty, K., Steketee, M., Fagan, A., Hanson, K., & Hawkins, J. D. (2008). Communties that care, core elements and context: Research of implementation in two countries. Social Development Issues, 30 (3), 42-58.
Jonkman, H., (2015) Communities That Care in Niedersachsen. Ergebnisse der Implementation von CTC in fünf Standorten (2013-2014), Hannover: LPR
Kandel, D. and Kandel, E. (2015), ‘The Gateway Hypothesis of substance abuse: developmental, biological and societal perspectives’, Acta Paediatrica 104(2), 130-137, doi: 10.1111/apa.12851.
Kim, B.K., Gloppen, K.M., Rhew, I.C., Oesterle, S., Hawkins, J.D. (2014), ‘Effects of the Communities That Care prevention system on youth reports of protective factors’, Prevention Science, 16(5), pp. 652-662.
Kuklinski, M.R., Briney, J.S., Hawkins, J.D. and Catalano, R.F. (2012), ‘Cost benefit analysis of Communities That Care outcomes at eighth grade’, Prevention Science 13(2), pp. 150-161.
Kuklinski, M.R., Hawkins, J.D., Plotnick, R.D., Abbott, R.D. and Reid, C.K. (2013), ‘How has the economic downturn affected communities and implementation of science based prevention in the randomized trial of Communities That Care?’, American Journal of Community Psychology 51(3-4), pp. 370-384.
Kuklinski, M.R., Fagan, A.A., Hawkins, J.D., Briney, J.S. and Catalano, R.F. (2015), ‘Benefit cost analysis of a randomized evaluation of Communities That Care: monetizing intervention effects on the initiation of delinquency and substance use through grade 12’, Journal of Experimental Criminology 11(2), pp. 165-192.
Leshner, A.I. (1997), ‘Drug abuse and addiction treatment research: the next generation’, Archives of General Psychiatry 54, pp. 691-694.
Leshner, A.I. (1999), ‘Science based views of drug addiction and its treatment’, JAMA 282, pp. 1314- 1316.
van Leeuwen, A.P., Verhulst, F.C., Reijneveld, S.A., Vollebergh, W.A., Ormel, J. and Huizink, A.C. (2011), ‘Can the gateway hypothesis, the common liability model and/or, the route of administration model predict initiation of cannabis use during adolescence? A survival analysis — the TRAILS study’, Journal of Adolescent Health 48, pp. 73-78.
Mak, J., Huygen, A., Steketee, M., Jonkman, H. (2009) Opgroeien in veilige wijken Evaluatie van Communities that Care in Maassluis, Hoogvliet en Leiden-Stevenshof. Verwey-Jonker Instituut, Utrecht.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G. and the PRISMA Group (2009), ‘Preferred reporting items for systematic reviews and meta analyses: the PRISMA statement’, PLoS Medicine 6(7), p. e1000097.
Moss, H.B., Chen, C.M. and Yi, H.Y. (2014), ‘Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample’, Drug and Alcohol Dependence 136, pp. 51-62.
Monahan, K.C., Hawkins, J.D. and Abbott, R.D. (2013), ‘The application of meta analysis within a matched pair randomized control trial: an illustration testing the effects of Communities That Care on delinquent behavior’, Prevention Science 14(1), pp. 1-12.
Morojele, N.K., Muller, M., Reddy, P., Lombard, C.J., Flisher, A.J. and Ziervogel, C.F. (2002), ‘Measurement of risk and protective factors for drug use and anti social behavior among high school students in South Africa’, Journal of Drug Education 32(1), pp. 25-39.
Murray, D.M., Van Horn, M.L., Hawkins. J.D. and Arthur, M.W. (2006), ‘Analysis strategies for a community trial to reduce adolescent ATOD use: a comparison of random coefficient and ANOVA/ ANCOVA models’, Contemporary Clinical Trials 27(2), pp. 188-206.
Oesterle, S., Hawkins, J.D., Fagan, A.A., Abbott, R.D. and Catalano, R.F. (2010), ‘Testing the universality of the effects of the Communities That Care prevention system for preventing adolescent drug use and delinquency’, Prevention Science 11(4), pp. 411-423.
Oesterle, S., Hawkins, J.D., Fagan, A.A., Abbott, R.D. and Catalano, R.F. (2014), ‘Variation in the sustained effects of the Communities That Care prevention system on adolescent smoking, delinquency, and violence’, Prevention Science 15(2), pp. 138-145.
Oesterle, S., Hawkins, J.D., Kuklinski, M.R., Fagan, A.A., Fleming, C., Rhew, I.C., Brown, E.C. et al. (2015), ‘Effects of Communities That Care on males’ and females’ drug use and delinquency 9 years after baseline in a community randomized trial’, American Journal of Community Psychology 56(3- 4), pp. 217-28.
Quinby, R.K., Hanson, K., Brooke Weiss, B., Arthur, M.W., Hawkins, J.D. and Fagan, A.A. (2008), ‘Installing the Communities That Care prevention system: implementation progress and fidelity in a randomized controlled trial’, Journal of Community Psychology 36(3), pp. 313-332.
Rhew, I.C., Monahan, K.C., Oesterle, S. and Hawkins, J.D. (2016), ‘The Communities That Care brief depression scale: psychometric properties and criterion validity’, Journal of Community Psychology 44(3), pp. 391-398.
Shakeshaft, A., Doran, C., Petrie, D., Breen, C., Havard, A., Abudeen, A., Harwood, E. et al. (2014), ‘The effectiveness of community action in reducing risky alcohol consumption and harm: a cluster randomised controlled trial’, PLoS Medicine 11(3), p. e1001617.
Shapiro, V.B., Hawkins, J.D., Oesterle, S., Monahan, K.C., Brown, E.C. and Arthur, M.W. (2013), ‘Variation in the effect of Communities That Care on community adoption of a scientific approach to prevention’, Journal of the Society for Social Work and Research 4(3).
Scholes Balog, K.E., Hemphill, S., Reid, S., Patton, G. and Toumbourou, J. (2013), ‘Predicting early initiation of alcohol use: a prospective study of Australian children’, Substance Use & Misuse 48(4), pp. 343-352.
Shapiro, V.B., Oesterle, S., Abbott, R.D., Arthur, M.W. and Hawkins, J.D. (2013), ‘Measuring dimensions of coalition functioning for effective and participatory community practice’, Social Work Research 37(4), pp. 349-359.
Shapiro, V.B., Hawkins, J.D. and Oesterle, S. (2015), ‘Building local infrastructure for community adoption of science based prevention: the role of coalition functioning’, Prevention Science 16, p. 1136.
Steketee, M., Mak, J., Huygen, A. (2006) Opgroeien in veilige wijken. Communities that care als instrument voor lokaal preventief jeugdbeleid. Van Gorkum.
Steketee, M., Oesterle, S., Jonkman, H., Hawkins, J.D., Haggerty, K.P. and Aussems, C. (2013), ‘Transforming prevention systems in the United States and the Netherlands using Communities That Care Promising prevention in the eyes of Josine Junger Tas’, European Journal on Criminal Policy and Research 19(2), pp. 99-116.
Schubert, H., K. Veil, H. Spieckermann und S. Abels (2013) Evaluation des Modellprojektes „Communities That Care“ in Niedersachsen: Theoretische Grundlagen und empirische Befunde zur sozialräumlichen Prävention in Netzwerken, Köln.
Trenz, R.C., Scherer, M., Harrell, P., Zur, J., Sinha, A. and Latimer, W. (2012), ‘Early onset of drug and polysubstance use as predictors of injection drug use among adult drug users’, Addictive Behaviors 37(4), pp. 367-372.
West, R. (2013), Models of addiction, EMCDDA Insights 14, Publications Office of the European Union, Luxembourg.
West, R. and Brown, J. (2013), Theory of addiction, 2nd edition, Wiley Blackwell, London.
Winters, K.C. and Lee, C.Y. (2008), ‘Likelihood of developing an alcohol and cannabis use disorder during youth: association with recent use and age’, Drug and Alcohol Dependence 92(1-3), pp. 239-247.Van Horn, M.L., Fagan, A.A., Hawkins, J.D. and Oesterle, S. (2014), ‘Effects of the Communities That Care system on cross sectional profiles of adolescent substance use and delinquency’, American Journal of Preventive Medicine 47(2), pp. 188-197, doi:10.1016/j.amepre.2014.04.004.
Wongtongkam, N., Ward, P.R., Day, A. and Winefield, A.H. (2014), ‘The influence of protective and risk factors in individual, peer and school domains on Thai adolescents’ alcohol and illicit drug use: a survey’, Addictive Behaviors 39(10), pp. 1447-1451